
CIENCIAS AGRARIAS-Reporte de Caso
TRAUMATIC CONSTRICTIVE PERICARDITIS IN A HORSE PERICARDITIS CONSTRICTIVA POR TRAUMA EXTERNO EN UN EQUINO
Teresa Oviedo S.1, Misael Oviedo P.2, José R. Martínez A.3*
1MV, M.Sc., cPhD. Profesora Departamento de Ciencias Pecuarias, Carrera 6, No. 76-103, Universidad de Córdoba, Montería, Colombia. tere_oviedo@yahoo.com
2MV, M.Sc., cPhD. Departamento de Medicina Veterinária Preventiva, Av. Antônio Carlos 6627, Pampulha, Universidad Federal de Minas Gerais (UFMG), Belo Horizonte, Brasil. m_oviedo2000@yahoo.com
3MVZ, M.Sc., PhD. Profesor Escuela de Medicina Veterinaria, Facultad de Ciencias Agrarias, Universidad de Antioquia, Grupo de investigación Centauro. Carrera 75, No. 65-87, Ciudadela Robledo, Medellín, Colombia. * jrramonmvz@yahoo.com
Rev. U.D.C.A Act. & Div. Cient. 17(1): 293-297, Enero-Junio, 2014
INTRODUCTION
Pericarditis is an inflammatory condition of the outer layer of the heart, the pericardium. It has been related to different etiologies, including bacterial and viral infections (May et al. 2002; Perkins et al. 2004; Bolin et al. 2005), traumas (Bertone & Dill, 1985), neoplasias (Stoica et al. 2004) and secondary to inflammatory processes in adjacent organs or septicemia (Benson & Sweeney, 1984; Jesty & Reef, 2006). Idiopathic or immunological causes are also described, such as eosinophilic and inflammatory sterile effusions (Worth & Reef, 1998; Bonagura & Reef, 2005). Likewise, outbreaks of seasonal pericarditis have been described in horses related to migrating worms (Malacosoma americanum) in some regions of the USA, although the causes have not been clarified (Seahorn et al. 2003; Jones et al. 2007; Sebastian et al. 2008).
Traumatic pericarditis is more frequently presented in bovines and originates from the penetration of metallic sharp objects through the reticular wall, diaphragm, pericardium and, sometimes, the myocardium (Radostis et al. 2007). Pericarditis is an uncommon pathology in horses (Rooney & Robertson, 1996), in particular the traumatic one. This report describes the occurrence of pericarditis caused by a perforating thoracic trauma, and diagnosed on the necropsy.
Patient examination
Anamnesis and clinical findings:
A necropsy service was required for a two year old mixedbreed female horse. The animal had suffered a perforation in the thoracic area with a wood splinter when it jumped over a fence 1.5 months earlier. At the time, the horse caretaker had sutured and treated the wound topically; the animal also received antibiotics (22,000IU/kg/im/bid procaine penicillin) and an anti-inflammatory (phenylbutazone 4.4mg/kg/iv/sid) for one week. According to the caregiver the animal exhibited anorexia, intense dyspnea, reluctance to movement and abdominal strain for days prior to its death.
Necropsy findings
The most important injures found in the necropsy were the presence of a scar on the ventral thoracic wall (Figure 1A), and the presence of yellowish areas indicating fibrin in the subcutaneous tissue of the thorax. Also, severe pulmonary and pleural congestion were found, as well as the presence of serosanguineous fluid in the thoracic cavity (hydrothorax) (Figure 1B); besides a hypertrophied heart, the pericardial sac was notably thickened and adhered to the epicardium. On the epicardial surface of the heart, a thick fibrin layer was noticed (Figure 1C). The abdominal cavity presented an abundant quantity of yellowish fluid (ascites) (Figure 1D) and the liver was congested and enlarged.
DISCUSSION
It is always difficult to determine the cause of a pericardial inflammation based on the macroscopic examination of an injury. For this reason, a morphologic classification is commonly used (Mexie & Robinson, 2007). Although, a traumatic pericarditis is a relatively common event in bovines (Radostis et al. 2007), different species can be also affected (Kolm et al. 2001; Torki et al. 2011), but in horses there are few cases of the traumatic pericarditis. One dates from 1985 (Bertone & Dill, 1985), related to the ingestion of a metallic foreign body that moved from the stomach producing a restrictive pericarditis, described as a case of gastro pericarditis.
Even though there was no ingestion of any foreign body, it is valid to consider this case like being of a traumatic origin, since it is directly related to the perforation in the thorax of the animal while jumping over a wood fence. However, cytological and microbiological studies of the fluids found in this case were not made to further diagnose the infectious pathogens.
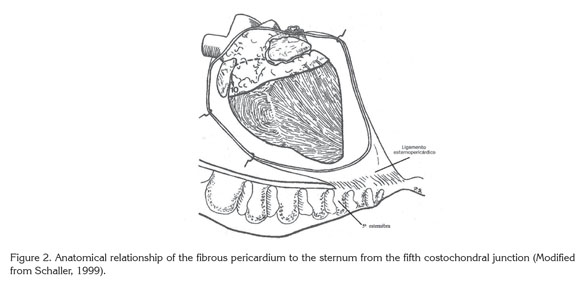
In the horse anatomy, the ventral area of the fibrous pericardium is attached to the sternum by the sternopericardial ligament, from its fifth costochondral junction to the xiphoid process (Schaller, 1999; Barone, 1993) (Figure 2). Evaluating the scar on the ventral thoracic wall of the animal, it was obvious that the injury reached a point between the fifth and the sixth costochondral junction. Considering the close anatomical relation that this region has with the pericardium, it is likely that the trauma initiated the inflammatory process.
Sojka et al. (1990) reported one case with similar pathogeny of septic pericarditis in a cow in which the cause was related to the penetration of a wire through the skin and the sternum, finally reaching the pericardium. Davis et al. (2002), in a retrospective study, described pleural and pericardial effusion in a horse as a result of a trauma on the left side of the thorax, despite the intensity of the trauma was not specified. This proves the sensitivity of this area because of the proximity of the cardiac silhouette to the thoracic wall.
The sternal bone marrow aspiration technique is considered an innocuous procedure. However, Jacobs et al. (1983) related the death of a horse after an sternal bone marrow aspiration, and in the necropsy it was found that the cause of the death was the restriction of diastolic filling (cardiac plugging) resulting from a small laceration on the left ventricle during a biopsy. Similarly, Durando et al. (2006) described a case of non-lethal pneumopericardium during a sternal bone marrow aspiration in a horse. Though those cases are rare, they probably resulted from a wrong assessment of the topographical anatomy of the aspiration area, therefore making mistakes when determining the right place and depth of needle insertion (Kasashima et al. 2011).
The anatomopathological findings suggest a case of constrictive pericarditis, characterized by extensive fibrosis and thickening of the pericardial sac as a sequel of inflammatory processes or presence of fibrin between the visceral and the parietal pericardium layers (Worth & Reef, 1998). The piercing trauma possibly reached the pericardium and caused substantial injuries to the adjacent structures. Constrictive pericarditis can decrease the ventricular filling and the diastolic function, compromising the cardiac function and causing a congestive cardiac failure (Bonagura & Reef, 2005).
Davis et al. (2002) have studied cases of congestive cardiac failure in horses and they have found that this condition can be associated, among other causes, to pericarditis. In addition, they concluded that this is a rare condition in horses and the prognosis is serious in the long term. These statements are compatible with the case related in this article, in which some injuries took place as a consequence of a pronounced left and right sided cardiac failure, such as hypertrophy, congestion in diverse organs, hydrothorax and ascites, as well as the death of the animal, for cause of the congestive cardiac failure.
Finally, in the dynamic of the evolution of the clinical symptoms, the initial presence of infecting microorganisms from the penetration in the wound must not be ruled out. After this, it took place the beginning of an inflammatory process and the subsequent origin of pericardial effusion and fibrinous pericarditis that caused cardiac plugging and constriction, leading to an eventual congestive cardiac failure, once all the initial compensatory mechanisms were exhausted (Reef & McGuirk, 2009). Unfortunately, it was not possible to correlate all the clinical sings since the very specific moment of the accident, owing to the way this case developed.
CONCLUSION
Traumatic pericarditis is an uncommon condition in horses. However, it must be seriously considered when there are any injures involving the thoracic wall close to the sternum, because of its anatomical proximity with the sternopericardial ligament. Any injure in this region of the horse body can lead to a complete cardiac failure, as seen in this particular case. It is recommended that equine practitioners perform ultrasonographic evaluation in patients with chest injuries of this nature.
Acknowledgements: To Dr. Germán Bohórquez Mahecha, Professor of Domestic Animal Anatomy, UFMG - ICB, for advising in anatomical concerns. University of Cordoba and University of Antioquia, Colombia. Conflicts of interest: The manuscript was prepared and revised by all authors, who declare the absence of any conflict, which could put the validity of the present results in risk.
BIBLIOGRAPHY
1. BARONE, R. 1993. Pericardio In: Bortolami, Callegari, E (EDS). Anatomia Comparata dei Mammiferi Domestici, Vol 5. Angiologia, Edagricole. (Bologna). p.69-96.
2. BENSON, C.E.; SWEENEY, C,R. 1984. Isolation of Streptococcus pneumoniae type 3 from equine species. J. Clin. Microbiol. (USA). 20:1028-1030.
3. BERTONE, J.J.; DILL, S.G. 1985. Traumatic gastropericarditis in a horse. J. Am. Vet. Med. Assoc. (USA). 187:742-743.
4. BOLIN, D.C.; DONAHUE, J.M.; VICKERS, M.L.; HARRISON, L.; SELLS, S.; GILES, R.C.; HONG, C.B.; POONACHA, K.B.; ROBERTS, J. SEBASTIAN, M.M.; SWERCZEK, T.W.; TRAMONTIN, R.; WILLIAMS, N.M. 2005. Microbiologic and pathologic findings in an epidemic of equine pericarditis. J. Vet. Diagn. Invest. (USA). 17:38-44.
5. BONAGURA, J.D.; REEF, V.B. 2005. Alteraciones del aparato cardiovascular In: Reed S.M.; Bbayly w.m.; Sellon, D.C. (eds) Medicina Interna Equina. 2da. ed. Loius Missouri: Saunders. (Missouri). p.393-506.
6. DAVIS, J.L.; GARDNER, S.Y.; SCHWABENTON, B.; BREU. HAUS, B.A. 2002. Congestive heart failure in horses: 14 cases (1984-2001). J. Am. Vet. Med. Assoc. 220:1512-1515.
7. DURANDO, M.M.; ZARUCCO, L.; SCHAER, T.P.; ROSS, M.; REEF, V.B. 2006. Pneumopericardium in a horse secondary to sterna bone marrow aspiration. Equine Vet. Educ. (USA). 18:75-79.
8. JACOBS, R.M.; KOCIBA, G.J.; RUOFF, W.W. 1983. Monoclonal gammopathy in a horse with defective hemostasis. Vet. Pathol. (USA). 20:643-647.
9. JESTY, S.A.; REEF, V.B. 2006. Septicemia and cardiovascular infections in horses. Vet. Clin. North Am. Equine Pract. (USA). 22:481-495.
10. JONES, S.L.; VALENSIZI, A.; SONTAKKE, S.; SPRAYBERRY, K.A.; MAGGI, R.; HEGARTY, B.; BREITSCHWERDT, E. 2007. Use of an insect cell culture growth medium to isolate bacteria from horses with effusive, fibrinous pericarditis: a preliminary study. Vet. Microbiol. (USA). 121:177181.
11. KASASHIMA, Y.; UENO, T.; TOMITA, A.; GOODSHIP, A.E.; SMITH, R.K. 2011. Optimisation of bone marrow aspiration from the equine sternum for the safe recovery of mesenchymal stem cells. Equine Vet. J. (USA). 43:288-294.
12. KOLM, U.S.; KOSZTOLICH, A.; HOEGLER, S.; KNEISSL, S. 2001. Canine Traumatic Pericarditis by an Esophageal Foreign Body. J. Vet. Cardiology (USA)). 3:17-21.
13. MAY, K.A.; CHERAMIE, H.S.; HOWARD, R.D.; DUESTERDIECK, K.; MOLL, H.D.; PLEASANT, R.S.; PILE, RL. 2002. Purulent pericarditis as a sequela to clostridial myositis in a horse. Equine Vet. J. 34:636640.
14. MEXIE, M.G.; ROBINSON, W.F. 2007. Cardiovascular system. In: MAXIE M.G. (Ed.), JUBB, KENNEDY AND PALMER'S Pathology of Domestic Animals. Vol.3. 5th ed. Elsevier. (Philadelphia). p.22-23.
15. PERKINS, S.L.; MAGDESIAN, K.G.; THOMAS, W.P.; SPIER, S.J. 2004. Pericarditis and pleuritis caused by Corinebacterium pseudotuberculosis in a horse. J. Am. Vet. Med. Assoc. 224:1133-1138.
16. RADOSTIS, O.M.; GAY, C.C.; HINCHCLIFF, K.W.; CONSTABLE, P.D. 2007. Veterinary medicine: a textbook of the diseases of cattle, sheep, pigs, goats and horses. 10th ed. London: W.B Saunders (London). p.430-431.
17. REEF, V.B.; McGUIRK, S.M. 2009. Disease of the cardiovascular system. In: BP. Editors. Large Animal Internal Medicine. Fourth Edition. Louis Missouri, MosbyElsevier (Missouri). p.453-486.
18. ROONEY, J.R.; ROBERTSON, J.L. 1996. Equine Pathology, 1a edição. Iowa State University Press. (Iowa). p. 11.
19. SCHALLER, O. 1999. Nomenclatura Anatômica Veterinária Ilustrada, Editora Manole Ltda. São Paulo, 1a ed. Bras. (São Paulo). p.235-235.
20. SEAHORN, J.L.; SLOVIS, N.M.; REIMER, J.M.; CAREY, V.J.; DONAHUE, J.G.; COHEN, N.D. 2003. Casecontrol study of factors associated with fibrinous pericarditis among horses in central Kentucky during spring 2001. J. Am. Vet. Med. Assoc. 223:832-838.
21. SEBASTIAN, M.M.; BERNARD, W.V.; RIDDLE, T.W.; LATIMER, C.R.; FITZGERALD, T.D.; HARRISON, L.R. 2008. Mare Reproductive Loss Syndrome. Vet. Pathol. 45:710-722.
22. SOJKA, J.E.; WHITE, M.R.; WIDMER, W.R.; ALSTINE, W.G. 1990. An unusual case of traumatic pericarditis in a cow. J. Vet. Diagn. Invest. 2:139-142.
23. STOICA, G.; COHEN, N.; MENDES, O.; KIM, H.T. 2004. Use of immunohistochemical marker calretinin in the diagnosis of a diffuse malignant metastatic mesothelioma in an equine. J. Vet. Diagn. Invest. 16:240-243.
24. TORKI, E.; MOKHBER, DEZFOLI, M.R.; SASANI, F.; BAGHBAN, F.; SHAHABI, M.; MOTAGHINEJAD, M. 2011. Traumatic reticulo-pericarditis (trp) in sheep: a report of 4 cases in a herd. Slov. Vet. Res (Slovenian). 48:45-50.
25. WORTH, L.T.; REEF, V.B. 1998. Pericarditis in horses: 18 cases (1986-1995). J. Am. Vet. Med. Assoc. 212:248-253.
Recibido: Octubre 3 de 2013 Aceptado: Diciembre 2 de 2013

Revista U.D.C.A Actualidad & Divulgación Científica por Universidad de Ciencias Aplicadas y Ambientales se distribuye bajo una Licencia Creative Commons Atribución-NoComercial 4.0 Internacional.